
Nordica Bone Care blog
Let’s Chat about osteoporosis
On World Osteoporosis Awareness Day this year, our community came together to connect & learn about osteoporosis, and enjoy a delicious calcium-rich cheese platter sponsored
On World Osteoporosis Awareness Day this year, our community came together to connect & learn about osteoporosis, and enjoy a delicious calcium-rich cheese platter sponsored

Am I in the risk group for osteoporosis? Osteoporosis is often referred to as a “silent disease” because it typically doesn’t cause noticeable symptoms until

Characteristics of Osteoporosis Osteoporosis is a disease characterised by low bone mass and structural deterioration of bone tissue, leading to increased fragility and susceptibility to
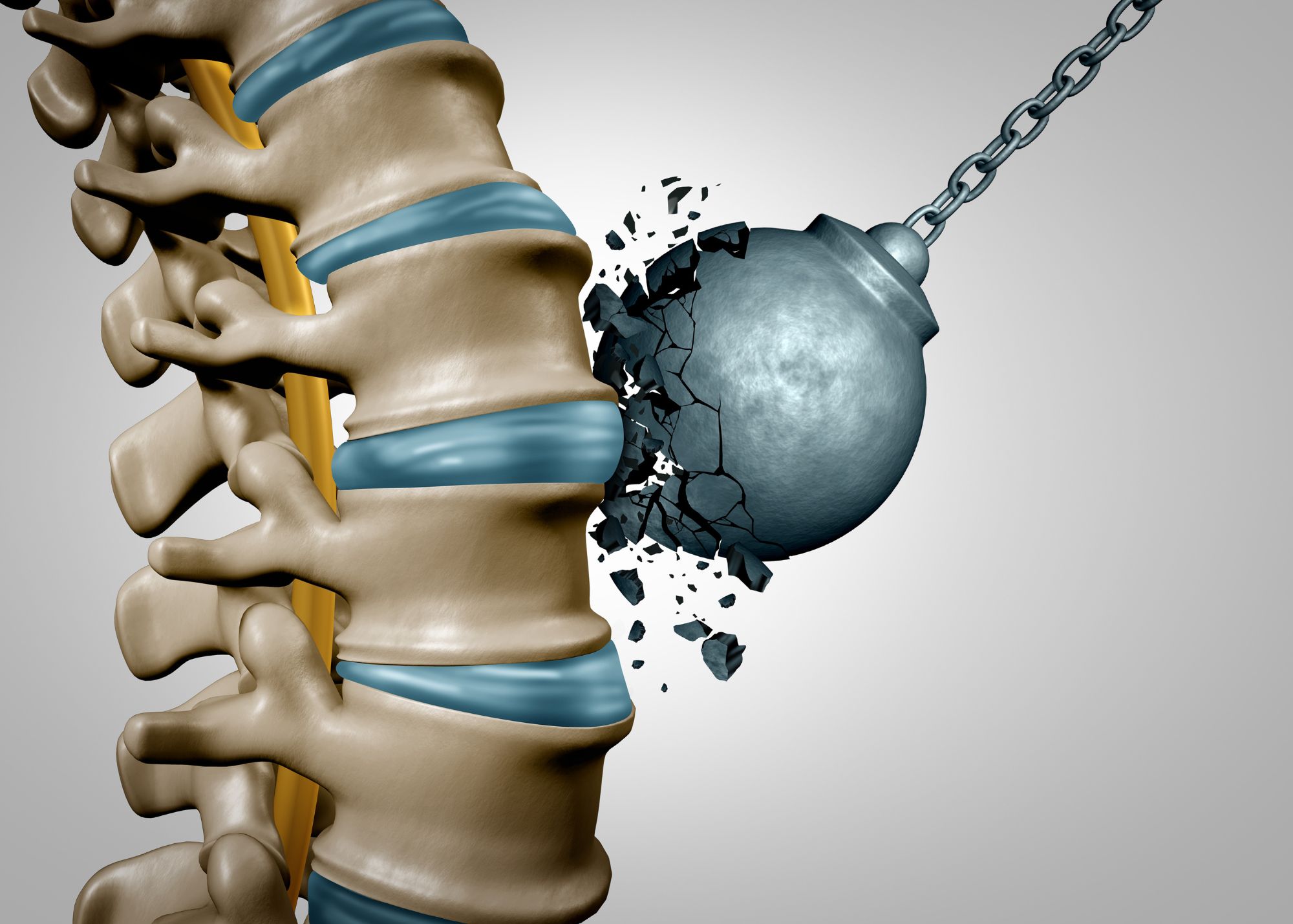
Bone strength is essential for maintaining a healthy skeletal system and plays a crucial role in supporting our body’s structure, protecting vital organs, and facilitating

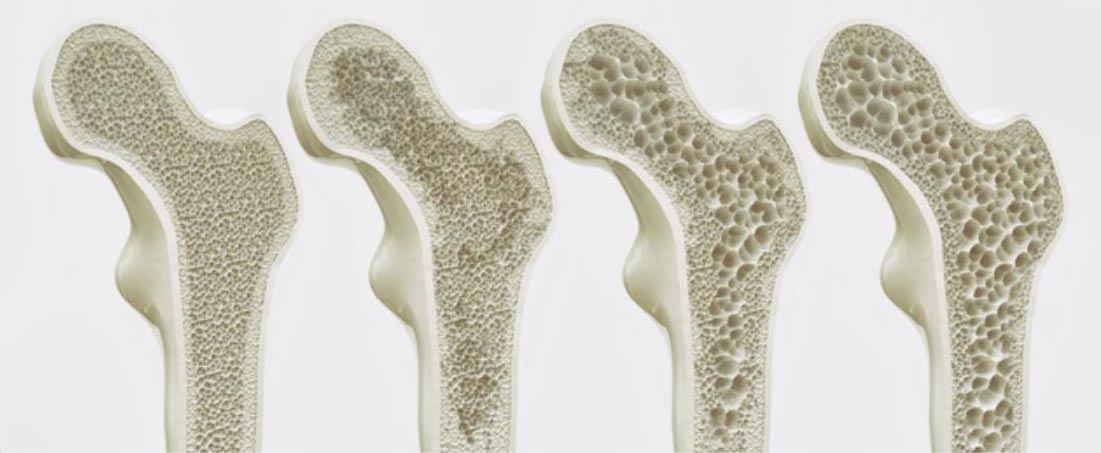
Are you curious about the structure and function of our bones? Understanding the anatomy and physiology of healthy bone tissue is essential to grasp the

Building Strength and Resilience with Osteoporosis Despite advancements in the diagnosis and treatment of osteoporosis, there is still much work to be done. Current protocols

What is the Osteoporosis Awareness Month? Throughout the month of May, we invite you to join us on a bone health journey. Together with our
Osteoporosis and Osteopenia: What You Need to Know What is osteoporosis? Osteoporosis is a condition that weakens the bones and increases the risk of low

Step Up For Bone Health Today, Thursday the 20th of October is world osteoporosis awareness day, and we joined the campaign Step Up For Bone
